
Stand up for a second if you can. Let your arms hang naturally. Don't adjust anything — just let your body land where it wants to land.
Now look in a mirror, or just feel it: is one shoulder sitting higher than the other? Does your head tilt, even slightly, toward one side? Does one side of your neck feel more compressed, more filled-in, more like there's less space there?
If you're like the majority of people I see in my practice, the answer is yes. And here's what's interesting: most people have noticed this. They've been told about it — a massage therapist mentioned it, or a chiropractor pointed it out, or they caught it in a photo and thought, huh, that looks uneven. And then they mostly filed it away as just the way they are.
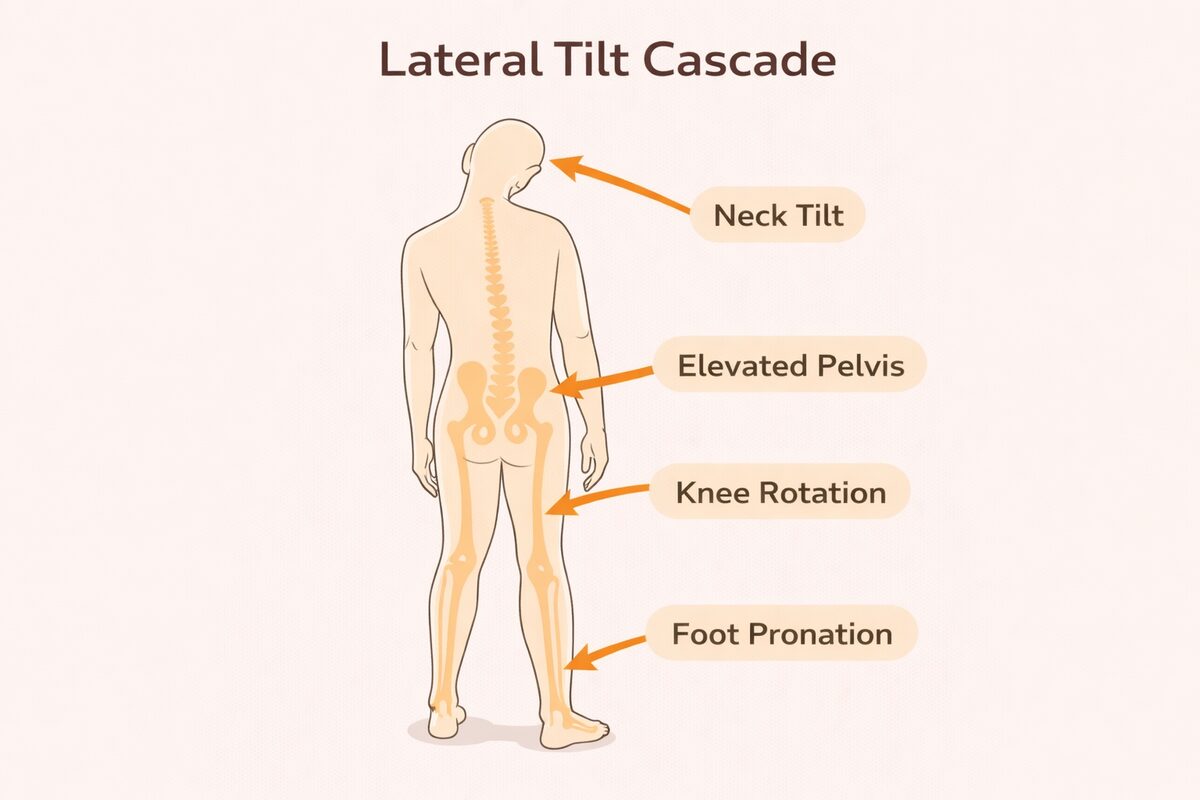
But lateral neck tilt — the subtle or not-so-subtle sideways shift of the head relative to the shoulders — isn't just cosmetic asymmetry. It's a postural compression pattern with a very specific downstream cascade. And once you understand what's actually happening in your body when one side collapses and the other compensates, the lopsided shoulder stops feeling like a curiosity and starts feeling like a story worth listening to.
How Lateral Tilt Creates Ipsilateral Compression
When the head tilts to one side — let's say it tilts right — a very predictable set of mechanical events unfolds. The right side of the body shortens. The scalenes, SCM, levator scapulae, upper trapezius, and intercostals on the right all approximate — they move closer together, reduce their length, and increase their tone. They're holding the collapse.
Simultaneously, the left side lengthens and weakens. The deep cervical flexors, the contralateral scalenes, the quadratus lumborum on the left — these muscles don't get shorter. They get longer. But longer doesn't mean stronger here. In the nervous system's logic, these muscles are inhibited. They're turned down to protect the system from pulling the already-tilted structure further out of balance.
This is the beginning of a chain reaction that travels through the entire body — from the right-side rib cage all the way to the right foot.
The side that collapses isn't the problem. It's the side that had to stop working — the inhibited side — that tells you where the real pattern lives.
The Full Downstream Cascade
Because the body is one continuous fascial system, a tilt at the top echoes through every structure below it. Here's what that looks like, zone by zone:
The Shoulder Blade That Does Everything Wrong
Here's where I want to go a bit deeper than most conversations about shoulder asymmetry go — because there's a specific mechanical story happening at the shoulder blade that I see constantly, and it's worth understanding clearly.
The scapula — your shoulder blade — is supposed to be a mobile, precise platform. When you raise your arm, it should glide upward and outward, rotating smoothly so the socket faces the direction your arm is moving. This movement is called scapular upward rotation, and it requires a very particular coordination between several muscles working together in sequence.
When lateral tilt and shoulder asymmetry are present, that coordination breaks down. And it breaks down in a predictable way — because the tonic muscles dominate early, and the phasic muscles that should be doing the stabilizing work get inhibited and show up late, or not at all.
Healthy shoulder movement requires a precise firing sequence: serratus anterior stabilizes the scapula against the ribcage, the lower trapezius pulls it upward and back, and the upper trapezius contributes rotation. These three need to work together, in the right order, at the right intensity.
What commonly happens instead: the levator scapulae and upper trapezius — both strong, tonic, chronically overactive muscles — fire first and dominate. The anterior deltoid engages hard and early to force the arm up. Meanwhile the serratus anterior and lower trapezius, which should be providing the stable foundation for all of this, are inhibited. They're quiet when they should be loud.
The result: the shoulder blade wings away from the ribs instead of tracking smoothly against them. The arm can get overhead, but at a cost — the wrong muscles are doing the work, the joint isn't centered, and the surrounding structures pay the price.
This is something I watch for constantly in clients, and it's one of the most common mechanical breakdowns I see in people who work with their bodies — but also in people who sit at desks all day, people who carry heavy bags on one side, people who breastfeed, people who sleep with one arm under their pillow. The pattern is remarkably consistent because the muscles involved are the same ones that tonic-phasic imbalance reliably disrupts.
In plain language: your shoulder blade is doing everything except what it's supposed to be doing. And the muscles that should be helping it — specifically the serratus anterior and lower trapezius — have essentially gone quiet.
A Real Pattern From the Treatment Room
I want to share a clinical picture from a recent client at Awaken Zen because it illustrates this pattern so precisely. Some details have been generalized to protect privacy, but the structural and mechanical picture is real and representative of what I see regularly.
This client came in with left shoulder pain rated 7 out of 10 during arm elevation — both abduction and flexion. Manual labor occupation: pushing, pulling, wrapping, overhead tasks with high repetitive load. Pain described as deep, near the posterior deltoid and triceps region. Right shoulder appeared more structurally depressed, left more painful — a classic bilateral asymmetry where the two sides are expressing the same pattern differently.
What I found on assessment: significant fascial densification in the anterior deltoid and lateral shoulder sleeve. Posterior deltoid fascia extremely tender and congested. Pectoralis minor shortened with an adhesive quality, driving anterior tilt and internal rotation of the left shoulder. Triceps long head dense and painful, restricting overhead reach. Scapulae showing reduced upward rotation and impaired posterior tilt. Thoracic spine stiff in extension. Breathing pattern: upper-chest dominant, shallow — maintaining chronic bracing in the pecs, scalenes, and upper traps.
The underlying picture: deltoid overload from a job that demands what the scapular stabilizers should be providing, but can't — because they've been inhibited by the dominant tonic muscles surrounding them. The levator scapulae was overactive and elevated the shoulder on effort, rather than the serratus and lower trap creating a smooth upward rotation track for the arm. The deltoid was compensating for a scapula that wasn't doing its job — recruiting harder to force range of motion that should have come for free with proper mechanics.
The plan was to release and decompress first — anterior and posterior deltoid fascia, pec minor, triceps long head — then improve thoracic mobility, then specifically facilitate the serratus and lower trapezius. The breathing pattern needed to shift before any of the downstream work would hold.
What I find so useful about cases like this is how clearly they illustrate something that's easy to say but takes time to really see: the pain is almost never where the problem is. This client's posterior deltoid was screaming. But the posterior deltoid was screaming because the serratus and lower trap had gone quiet. The pain was downstream. The origin was the inhibition upstream.
The Muscle Roles in Lateral Tilt Patterns
Here's how the tonic-phasic imbalance maps specifically to the lateral neck tilt and shoulder asymmetry pattern:
| Overactive — Holding the Collapse | Inhibited — Switched Off |
|---|---|
|
Levator scapulae
Elevates the shoulder on the compressed side; fires early and dominates overhead movement
|
Lower trapezius
Supposed to provide upward rotation and posterior scapular tilt; goes quiet
|
|
Upper trapezius
Recruited to substitute for proper serratus and lower trap coordination
|
Serratus anterior
The key scapular stabilizer against the ribcage; inhibited, allowing winging
|
|
Anterior deltoid
Overrecruited to compensate for a scapula that isn't tracking — takes on load it was never meant to carry
|
Infraspinatus / teres minor
External rotators of the shoulder; underactive, leaving internal rotation bias unchecked
|
|
SCM & ipsilateral scalenes
Shortening on the compressed side, holding the lateral tilt pattern in place
|
Deep cervical flexors
Contralateral stabilizers lengthen and weaken, losing the ability to create space
|
|
Right quadratus lumborum
Elevates the pelvis on the compressed side to maintain upright balance
|
Contralateral glute medius
Hip stabilizer on the long side weakens, unable to properly level the pelvis
|
The Archetype: "The Side-Shifter"
The Side-Shifter
"C-Shape Body Pattern"
One hip hiked, one shoulder depressed, spine curved into a C. The body has divided into two halves that aren't fully in conversation with each other — one side compressing, the other lengthening and giving up. Often this pattern emerges gradually, following years of one-sided repetitive work, a significant surgery or injury on one side, chronic one-sided carrying, or simply decades of habitual favoring.
The fascial signature is dense lateral lines — the tissue along the compressed side thickens and shortens — while cross-body spiral lines become congested and layered. The emotional signature tends toward compartmentalization: a felt sense of splitting, of holding two separate realities, of never quite being able to bring both sides of life into the same space at the same time.
When someone with this pattern receives bodywork, what they often feel is a profound sense of relief on the tight side — but also, sometimes, a surprising vulnerability on the long side. The long side has been quietly doing a lot of holding too. When it finally gets support, it can feel almost unfamiliar.
The Standing Habit That Gives It Away
One of the most reliable external signs of a lateral tilt and hip asymmetry pattern — outside the treatment room — is what someone does when they're just standing around. The position of comfort for this pattern is the contrapposto stance: weight shifted onto one hip, that hip popped out to the side, the opposite shoulder dropping. The spine forms a subtle C. The body looks relaxed, but what it's actually doing is unloading the compressed lateral chain by shifting load into the hip on one side.
Once you start noticing this, you see it constantly. The parent holding a child on one hip, always the same hip, for years. The store clerk who always weights their right side. The office worker who always crosses the same leg. The musician who always holds their instrument on the same shoulder.
None of these habits are inherently harmful in the short term. But repeated over months and years, the fascial system adapts around them. The pattern becomes structural. The adaptation becomes the default. And then one day there's pain — usually somewhere that seems unrelated to the habit — and the hunt for the source begins.
Is lateral tilt part of your pattern?
- When you look at your shoulders in a mirror, does one sit noticeably higher than the other?
- Do you consistently weight one hip when standing in line, at the kitchen counter, or waiting anywhere?
- Does one side of your neck feel more compressed or filled-in than the other?
- Has anyone ever told you that your shoulders are uneven, or that one side of your back is more developed?
- Do you get recurring tension or pain on one side of your upper back that never quite resolves?
- When you raise your arms overhead, does one side feel restricted or does one shoulder shrug up toward your ear involuntarily?
- Do you carry bags, children, or equipment consistently on the same side?
- Do you notice that one hip seems to sit higher in photos, or that your pants tend to slip more on one side?
What Helps — Starting With the Right Side First
The most important clinical principle for lateral tilt patterns is sequencing. Because the compressed side is holding the structure together, releasing it without first addressing the inhibited side creates instability. The body has no choice but to re-tighten. This is the most common reason why massage for these patterns doesn't hold — not because the massage was wrong, but because the inhibited side didn't get the activation it needed to pick up the load.
The correct sequence is: release the short side first, using slow sustained myofascial work, positional release, and decompression. Then activate the long side — the inhibited muscles that have been quietly not doing their job. Serratus anterior. Lower trapezius. Contralateral glute medius. Deep cervical flexors. These need to be woken back up and given clear neurological cues before the new position can hold.
For the shoulder specifically: the levator and upper trap need to soften before the serratus and lower trap can be meaningfully recruited. Trying to activate the serratus while the levator is still dominant is like trying to hear a quiet voice in a loud room — the signal gets drowned out. Create quiet first. Then introduce the signal.
And breath — always breath. The rib cage compression on the collapsed side changes how the diaphragm moves, which changes everything about how the thorax loads and what's available to the shoulder. Restoring lateral rib expansion on the compressed side is often the first thing that needs to happen before any of the shoulder work will fully land.
In Post 4, we shift from the side-to-side world into the rotational one — the spiral compression pattern that builds in people who habitually favor one side, and the helical torque it creates through the entire body. If lateral tilt is the body dividing into left and right, rotational compression is the body twisting — and the downstream effects are just as far-reaching.